Lessons from Beaconsfield
by Stuart Tierney
Introduction
In 2006, a large seismic event and fall of ground occurred at Beaconsfield Gold Mine (BGM) in northern Tasmania. One man, Larry Knight, was tragically killed and two other men, Todd Russell and Brant Webb, were trapped underground. The rockfall occurred while Russell and Webb were in the basket of a telehandler close to a stope brow. Knight was behind the telehandler retrieving mesh to install a backfill wall. The 800-tonne rockfall largely buried the telehandler and surrounding area but incredibly the men in the basket survived in a small pocket of air. Russell and Webb survived for five days before any contact was made with rescuers to confirm they were still alive. A small supply pipeline was established for food and water while a rescue tunnel was built to free them. They eventually escaped after 14 days underground.
The events at BGM sparked a worldwide media frenzy with more than 100 media organisations descending on the small town of less than 1,000 people. The moment Russell and Webb re-emerged on surface was a significant TV spectacle and there was a subsequent multi-million dollar bidding war for the rights to the story. The cultural impact is further demonstrated by the television movie “Beaconsfield” made to describe the events in 2012 and the Foo Fighters including a song called “Ballad of the Beaconsfield Miners” on their 2007 album.
Beaconsfield is an extraordinary human story of loss, survival, and a courageous rescue operation. Having said that, this post is going to focus on the geotechnical aspects of the incident and the events leading up to it. A lot has changed in the management of seismic risk in mines in the many years since Beaconsfield, so it is hard to see some of the circumstances repeated. We look back with the benefit of hindsight and the many advancements we have made in the analysis of seismicity and the design of seismic risk controls. But there are still some important lessons to be learned from these events and insights to be gained by considering the perspective of investigators that review major accidents. I will summarise the key geotechnical issues raised in the post-event investigations including the seismic analysis, mining method and sequencing, ground support systems and design methods, consultant management, risk assessment process, and communication problems.
I have used three main sources for this post that are publicly available that I have listed and linked below. There is a lot of detail in these reports that I have not included so they are still worth reading through if you have the time.
-
Chandler (2009). Findings, recommendations, and comments from the coroner’s inquest into the death of Larry Knight.
-
Melick (2007). Beaconsfield investigation report, prepared for the coroner.
-
Quinlan (2007). Annexure BD of the Beaconsfield investigation report. Report on occupational health and safety management at BGM.
Seismicity
The first signs of seismicity presented at BGM in 2002 during mining of the 760 m level (760 m below surface). The underground manager noted in a memo in June 2003 that seismic activity was increasing with depth. BGM engaged a consulting group in August 2003 to begin stress testing, and they reported in January 2004 that high deviatoric stress would be encountered below the 800 m level, particularly on the western end of the ore body. BGM adopted a rock noise reporting system in September 2003. By March 2006, 248 rock noise reports had been received and over half were falls of ground or rock spitting/bursting.
Other than one onsite Geotechnical Geologist, BGM largely relied on external consultants for geotechnical analysis and advice. One consultant began making regular visits to BGM in April 2004 when he recommended a seismic monitoring system be installed. An initial standalone SAQS system was installed consisting of a single seismometer and six uniaxial sensors. This was later replaced with a 12-channel ISS seismic system in August 2005. I have access to the data from the ISS system.
Two significant falls of ground occurred in October 2005, both related to large events. The second event was recorded as ML+1.9, the largest event at BGM to date. In response to these incidents, BGM suspended production and brought in multiple consultants to conduct various geotechnical assessments. Production was resumed in late January 2006 and there were no further large events above ML+1.0 until the main ML+2.3 event on 25 April 2006. The 25th of April is a public holiday and national day of remembrance in Australia and New Zealand known as Anzac Day.
Figure 1 shows the seismic data leading up to the Anzac Day event. Most of the seismicity is associated with the stoping on the western side of the orebody, particularly between the 735 and 965 m levels. The location of the Anzac Day event is indicated with a black marker and is close to the 925 m level where the main rockfall occurred.
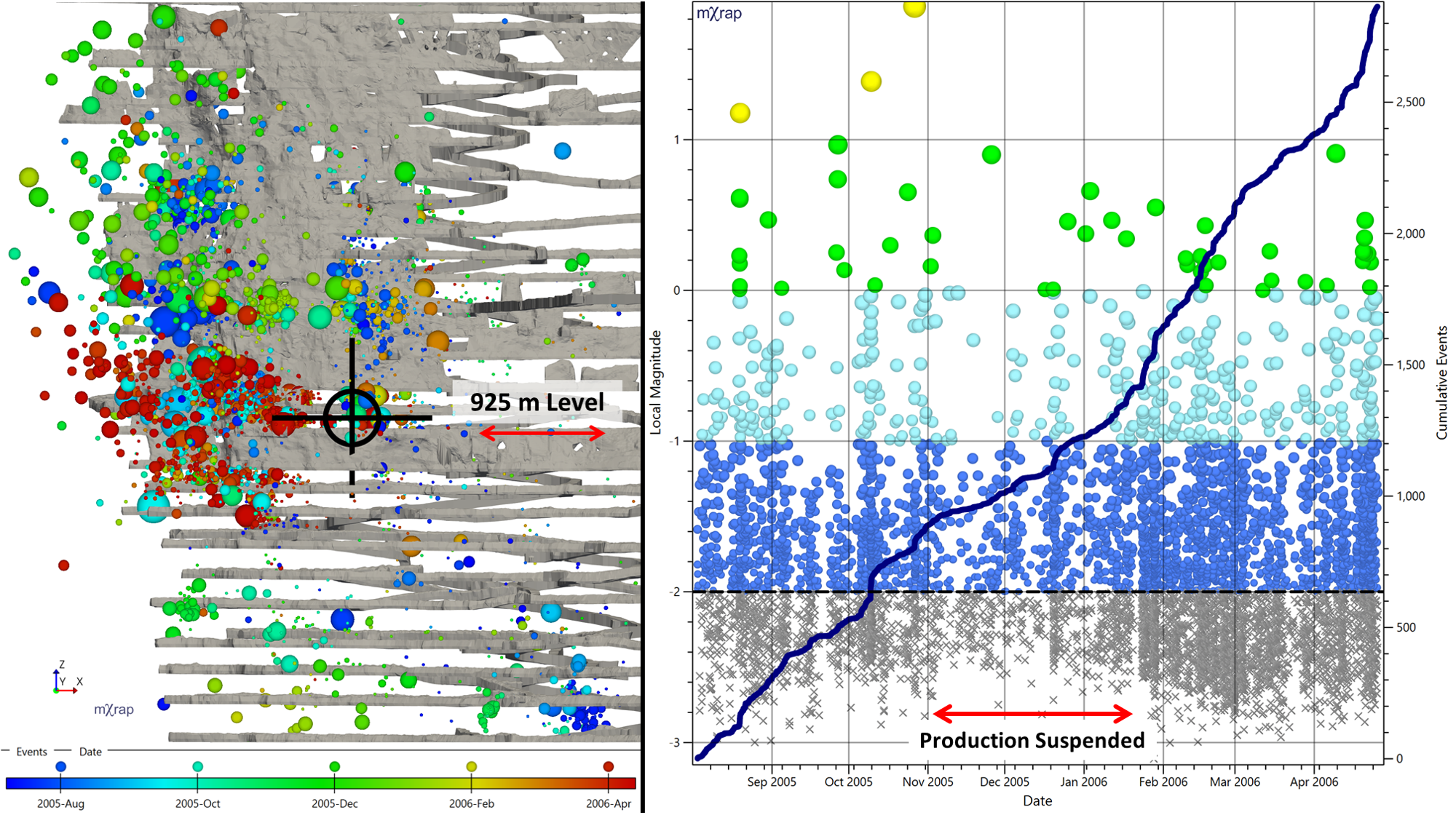
The post-event seismic investigation noted an increase in seismic activity with depth and an acceleration in the three months leading up to Anzac Day. Looking at the magnitude-time chart, the activity rate doesn’t seem too out of the ordinary. The drop in activity rate during the halt in production makes it seem like more of an increase.
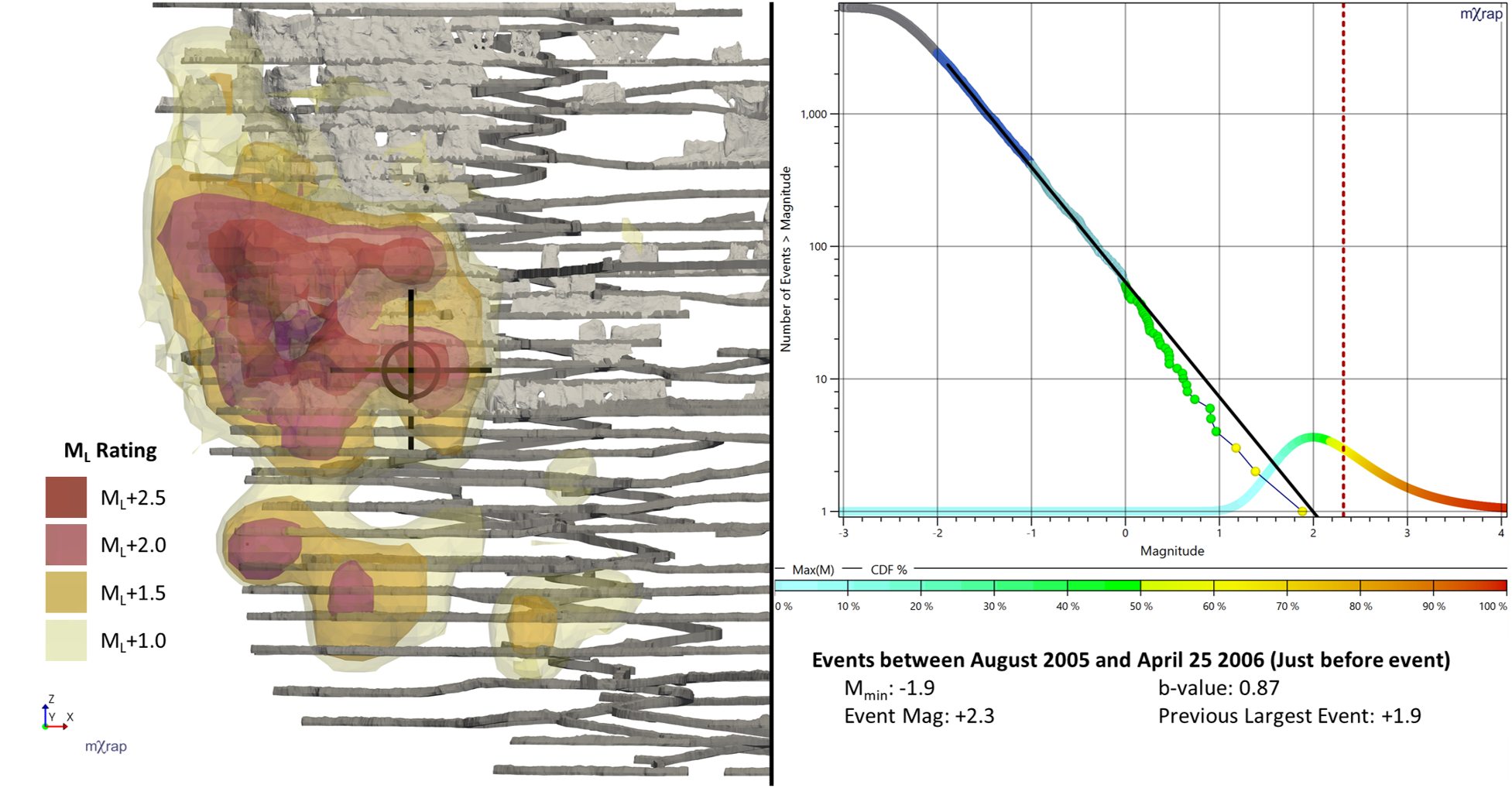
I have plotted a hazard assessment for the events prior to Anzac Day in Figure 2 (Note: the 3D hazard assessment tool was not available at the time, this analysis is retrospective). The location of the Anzac Day event is shown with a black marker, and the magnitude is shown with a vertical red dotted line on the frequency-magnitude chart. The seismic investigation presented to the coroner concluded that the environment at BGM was capable of producing events greater than ML+2.0. I agree that BGM’s seismic risk management plan should have been designed with the expectation of an event with a magnitude and location similar to that of the Anzac Day event. The magnitude is well within the expected range on the frequency-magnitude chart for the largest event and the location is in one of the main hazard hotspots. The timing of the event is another matter. It is good to see that the coroner seemed to understand this well, despite having no prior knowledge of seismicity in mines. He noted that “seismicity, by its nature, is a totally unpredictable beast so that the timing of a future significant event could not be predicted”. This does not mean however that it wasn’t incumbent upon BGM to have a full array of strategies to withstand the effects of such an event when it occurred. “The planning for these strategies needed, in my opinion, to allow for a seismic event up to 2.5 in magnitude and to assume that it could occur tomorrow.” (Chandler, 2009)
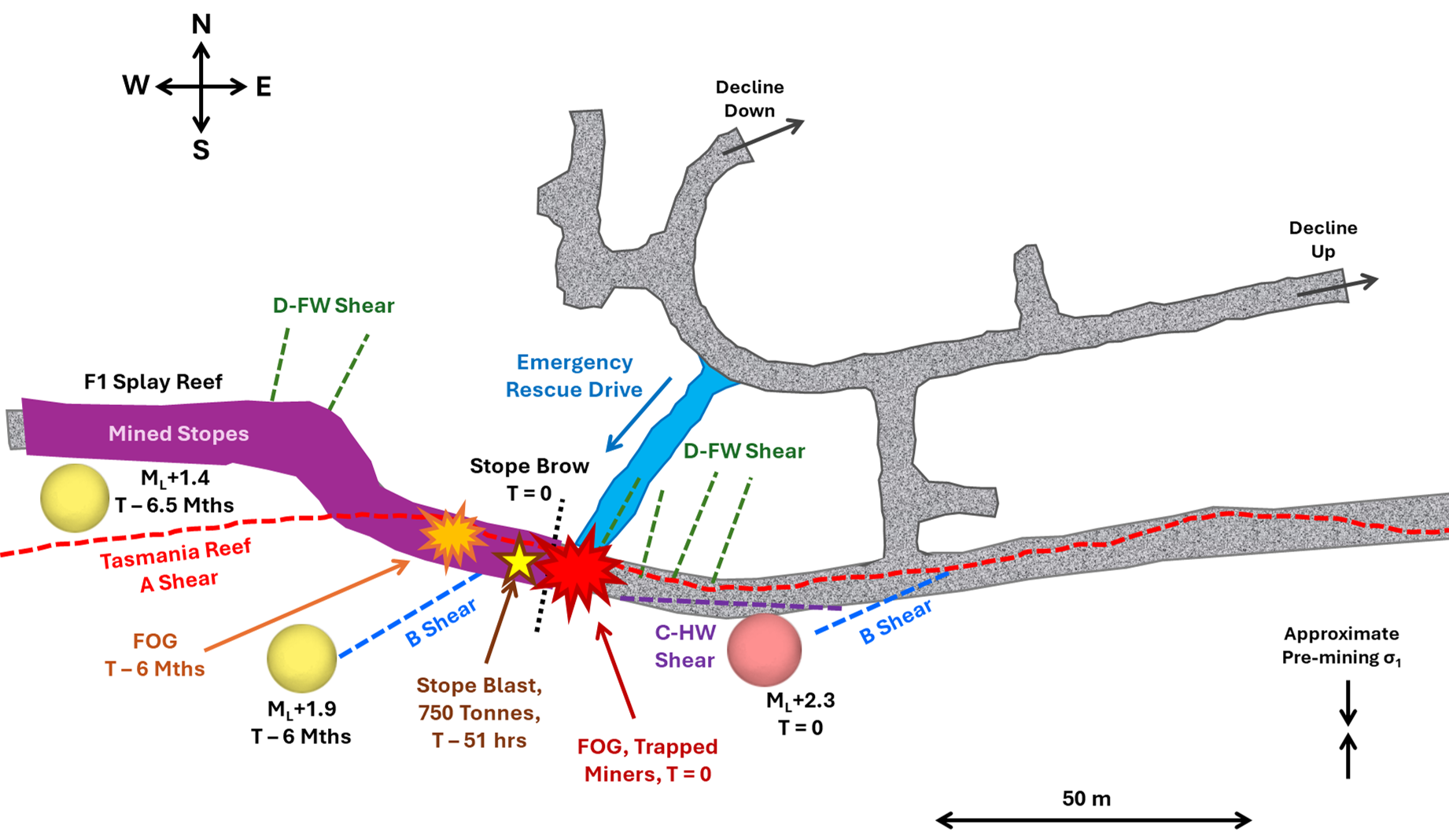
The seismic investigation attributed the Anzac Day event to slipping on the C-HW shear, a structure splaying off the main reef shear that runs along the ore drive. Figure 3 shows the major structures mapped on the 925 m level along with the recent large events and falls of ground. The Anzac Day fall of ground occurred close to the current stope brow. The most recent blast was two days earlier (approx. 51 hours before Anzac Day event). Another rockfall had occurred on this level slightly further to the west in October 2005, about six months before Anzac Day, along with a ML+1.9 event.
Mining Sequence
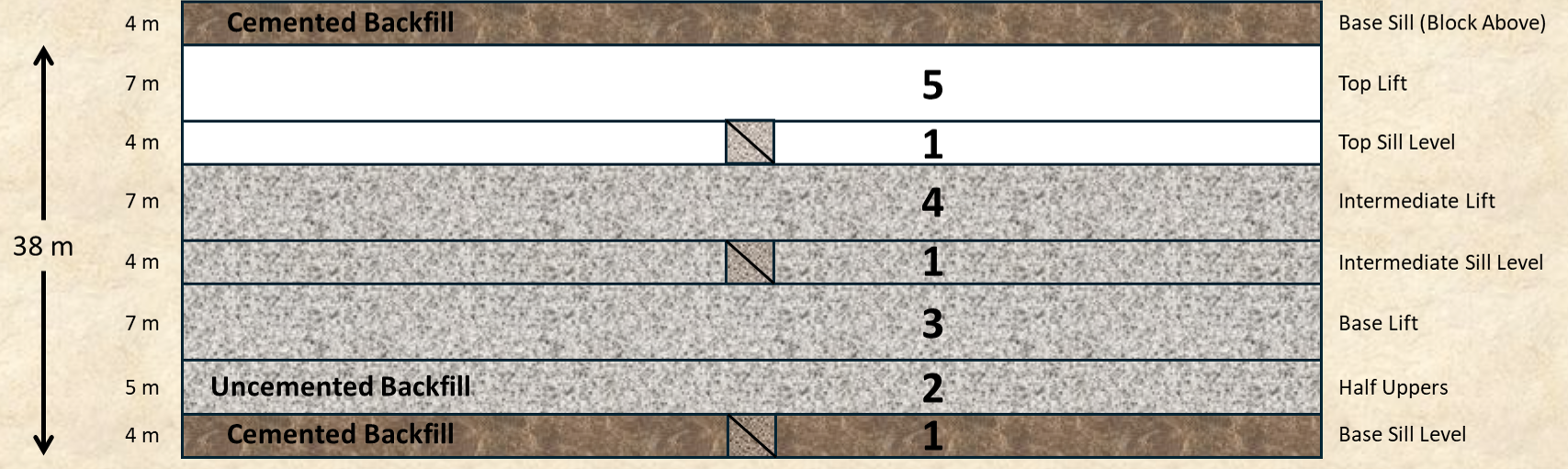
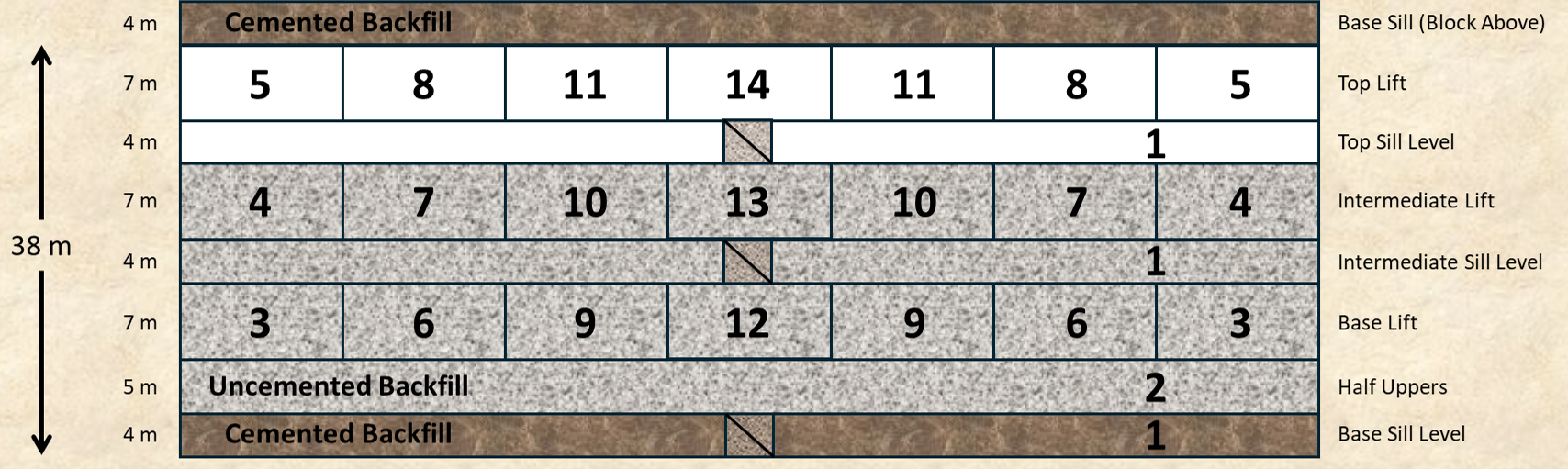
BGM were using the modified Avoca method for mining below the 840 m level. The sequence for this method consists of mining three levels as a block and is illustrated in Figure 4. The three sill drives are developed first, then half uppers are taken from the lowest level. This is then rehabilitated and the lower part of the drive is filled with cemented rock fill and cemented hydraulic fill to act as a working pad and to prevent dilution into the next block below. The rest of the lower level is extracted retreating towards the centre access and filled with uncemented waste rock. This is followed by the middle and upper levels. The upper level of the block is left unfilled.
The regular consultant advised BGM in early 2004 that the modified Avoca method was suitable for the 905 and 940 m blocks but a more conservative approach would be needed for deeper levels. The access at the 940 m level began development in March 2004 and the base lift and backfilling was completed by August 2005. Stoping had begun on the 925 m level when the October 2005 rockfalls occurred and production was suspended. The group of consultants collectively advised BGM to transition away from the modified Avoca method towards a checkerboard approach that retreats the three levels together (Figure 5). This method reduces the stress concentration along the top stoping level, reduces unsupported hanging wall spans, and adds confining fill earlier in the sequence. Unfortunately, the transition to the new sequence was already somewhat compromised since the 940 m level was already fully extracted.
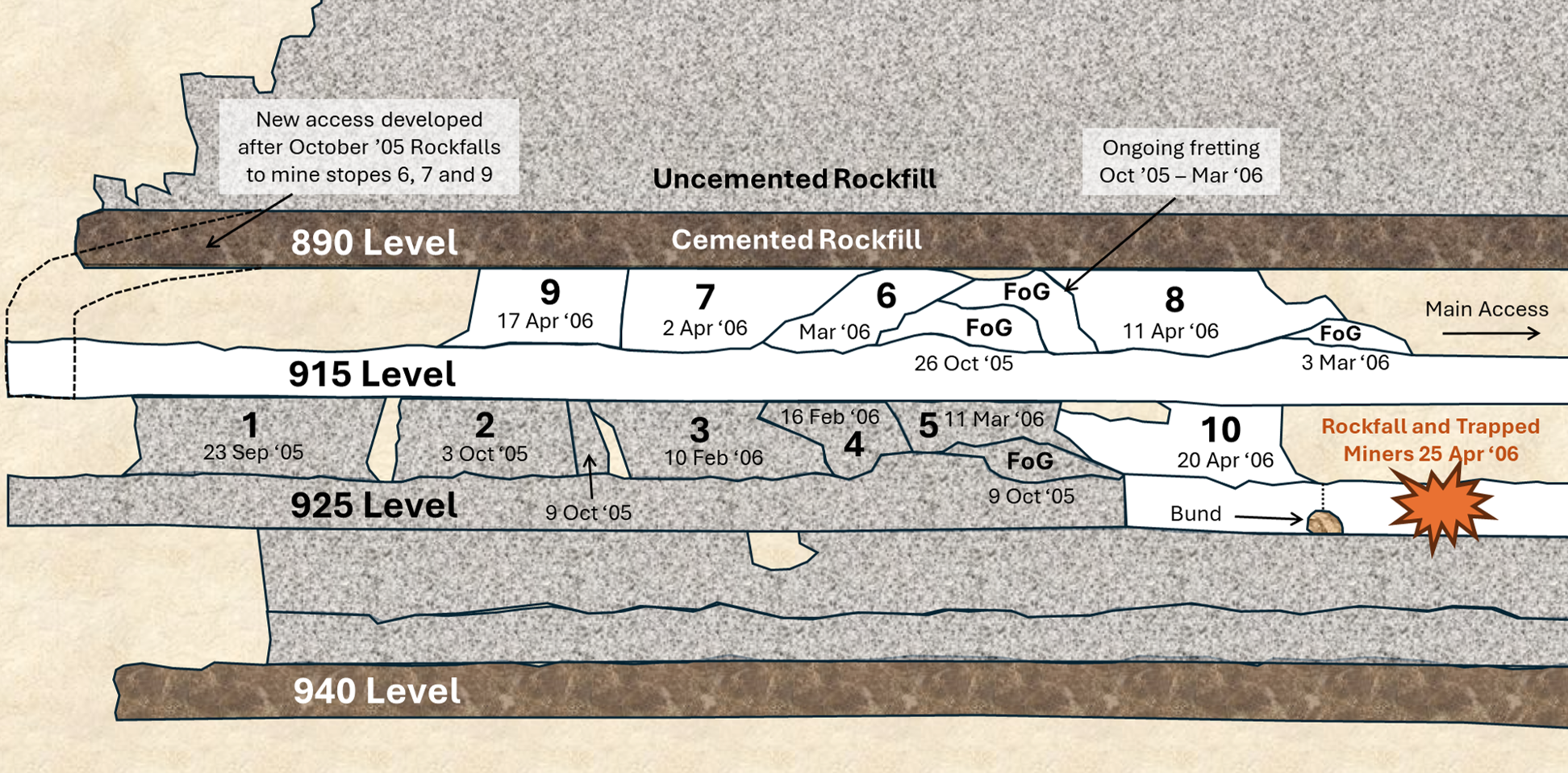
The falls of ground in October 2005 also complicated the transition to the new extraction sequence. The large rockfall on the 915 m level blocked access to the westernmost stopes and a new access was developed to mine stopes 6, 7, and 9 (Figure 6). The main controversy was the sequence reversal for stopes 8 and 10. In the normal checkerboard sequence, stope 10 on the 925 m level would have been mined first, backfilled, and then stope 8 would have been taken on the 915 m level. However, in late March 2006, poor ground conditions were observed on the 915 m level and BGM decided to reverse the sequence and mine stope 8 first.
BGM decided that if they mined stope 10 first, ground conditions would have deteriorated even further for mining stope 8 and that would have been a higher risk than mining in the planned sequence. There was another fall of ground on 3 March which likely contributed to the decision. Blasting stope 10 would have likely caused more spalling and made mining stope 8 even more difficult. The drawback of mining stope 8 first was that it increased the stress for mining stope 10. It also leaves a dual lift stope unfilled and reduces the local hanging wall confinement, potentially unclamping the shear structures parallel to the orebody.
The regular consultant and BGM management had different recollections on how the decision was made to reverse the sequence for stopes 8 and 10. BGM said that the change was proposed by the consultant during UG inspections on 28 March and everyone agreed it was the right decision at a debrief meeting the following day. The consultant did not recollect recommending a change of sequence and said that if he had, would have included it in his report and recommended additional ground support on the 925 m level for stope 10 (but not in the Anzac Day rock fall location).
The coroner reviewed the evidence and was not satisfied that the decision to reverse the sequence was made at the debrief meeting. He felt that it would have been mentioned in the underground managers personal notes for the meeting that he observed occupied a full page and were reasonably comprehensive. The coroner concluded that the decision was made by BGM management some time after the debrief meeting and they did not seek the consultant’s advice upon the possible impact of the sequence change on ground support in the area.
Although there may have been good reasons to reverse the sequence of stopes 8 and 10, the coroner was direct in his criticism of the decision making and risk assessment process of BGM. He commented that mining on the 915 and 925 m levels clearly required a cautious approach and “a properly documented and comprehensive evaluation of the risks associated with the proposed sequencing change. Such evaluation did not, in my opinion, occur” (Chandler 2009).
I think this is a good reminder of the importance of documenting key decisions. If an investigation occurs, everything is scrutinised. The coroner based his assessment on small notes left on UG inspection sheets, personal notes and how lengthy and comprehensive they were, email conversations, shift changeover notes etc. Even the rushed, informal notes you make may be relevant to an investigation. At minimum, for key decisions, it should be clear when the decision was made, who was involved in the decision, and the reasons behind the decision.
Ground Support
BGM introduced a rockfall incident reporting system in early 2004 where any fall of ground larger than one tonne or a failure of ground support was reported. In the period between February 2004 until the Anzac Day rockfalls in April 2006 there were 25 rockfalls reported. Many of the technical experts commented to investigators that the frequency and severity of recorded rockfalls was very high. Certainly by modern standards, it is a large number of rockfalls. Analysis of the rockfall reports show that:
- 64 % of rockfalls were greater than 50 tonnes (16 rockfalls)
- 72 % of rockfalls had failure depths greater than 1 m (18 rockfalls)
- 40 % of rockfalls had failure depths greater than 2 m (10 rockfalls)
- 60 % of rockfalls occurred from supported ground, a majority of these cases were in areas supported only by friction bolts and mesh
- Where ground support failed, 44 % were due to insufficient surface support, 24 % were due to bolts being too short, and 16 % were due to incorrect installation of support
The main reef unit that comprises the backs of the ore drives at BGM is strongly microfractured. In the early stages of development, the reef generally behaves as a massive rock unit. As mining progresses and stress increases, the reef tends to break along the existing microfractures. This can lead to a broken, cohesionless rock mass with very small block sizes, roughly 10 cm.
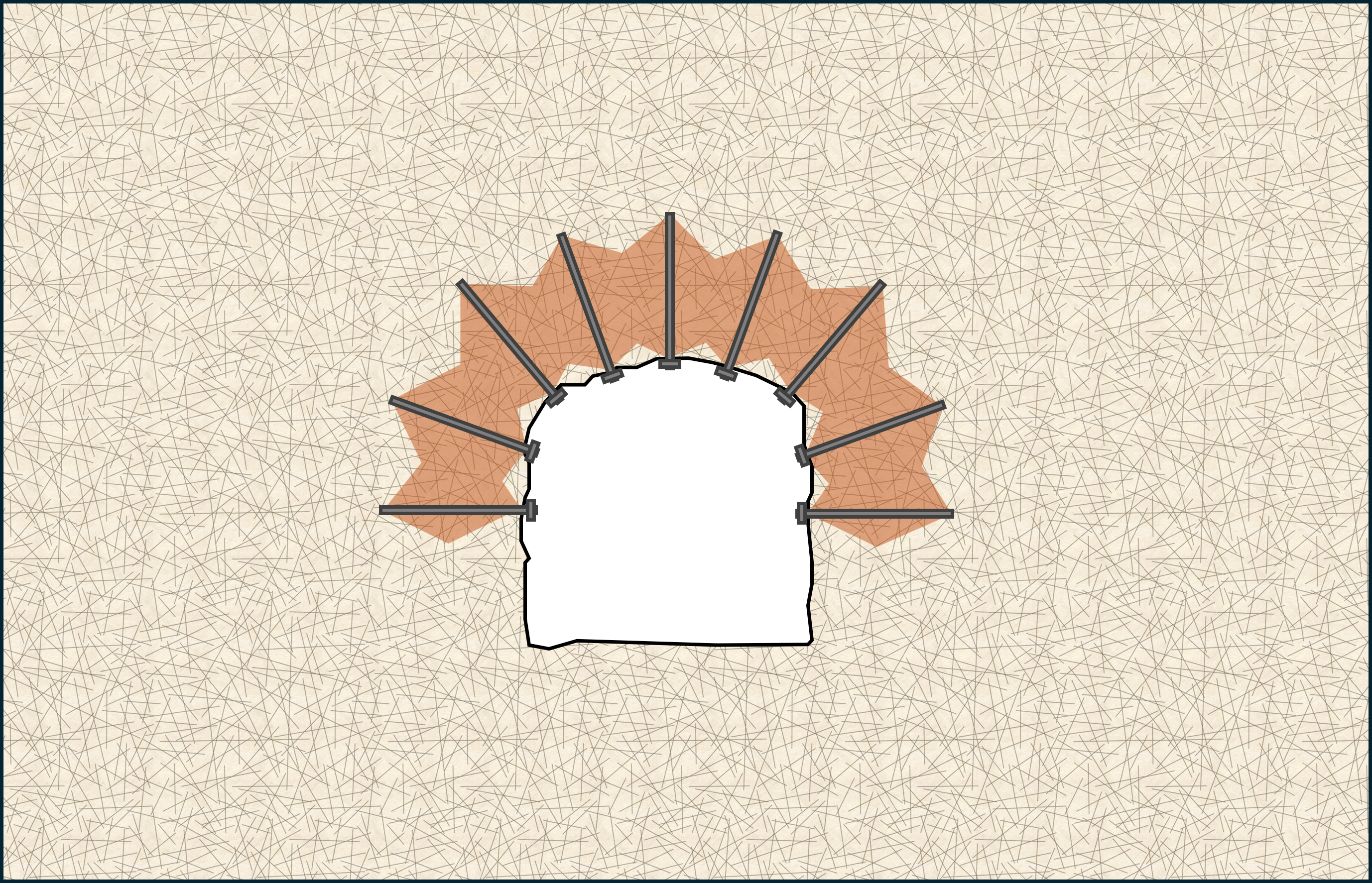
The standard ground support for ore drives at BGM consisted of split sets, welded mesh, and W-straps. Additional support was added to specific areas depending on conditions. Following the major rockfalls in October 2005, the regular consultant visited the mine and inspected the 915 and 925 m levels. He determined that the standard support was not sufficient to survive large seismic events. The falls of ground largely left the bolts intact with the rock mass unravelling around the bolts. He recommended additional cone bolts and straps installed along the 915 m level and resin-anchored threadbars with straps installed along the 925 m level. This recommendation was based on the idea that the 915 m level was expected to experience more significant stress damage, deformation, and seismicity with the planned sequence and therefore the more dynamic support units were installed there. The recommended support upgrades for both levels were installed by December 2005 including where the Anzac Day rockfalls occurred.
The documented foundation of the ground support design at BGM was the compressive arch theory (also known as the parabolic arch). This is the idea that the rock bolts create a zone of compression that binds together interlocking blocks, forms a self-supporting arch, and distributes the load to the abutments. However, the tendency of the main reef unit at BGM to form very small blocks means the rock bolts can’t maintain the compressive zone. The bolts need to be anchored into stable ground but there was a lot of history at BGM of rockfalls greater than 2 m depth. The rock bolts installed in the area were usually 2.4 m. The fall of ground on Anzac Day had a maximum depth of approximately 2.3 m.
One of the consultants that visited the mine after the October 2005 rockfalls brought up his concerns about the depth of failure and suggested installing cable bolts. He discussed his concerns with the regular consultant who had the view that longer bolts were not required and considered the ground to be too damaged for the installation of cable bolts. BGM interpreted the concerns about depth of failure to only be related to excavations greater than 6 m. The coroner found that interpretation illogical, given the BGM GCMP already provided for cable bolts to be used when the span of excavations was greater than 6 m.
BGM never formally addressed the disagreement between consultants regarding cable bolts and the depth of failure issue. They effectively deferred to the regular consultant who was both the original designer of the ground support and its auditor after the October 2005 rockfalls. The coroner was critical of this dynamic where the same person was effectively asked to “mark their own work.”
Of the six consultants to offer their view on the ground support design following the October 2005 rockfalls, only the regular consultant, the original designer, was firmly of the view that the compressive arch theory was suitable for the ground conditions at BGM. Most of the other consultants were concerned about the very small block size and depth of failure of previous rockfalls. The compressive arch theory also does not consider dynamic loading. In the coroner’s opinion, “the unsuitability of the compressive arch, or, in the very least questions as to its suitability should have become apparent to BGM following the October rockfalls” (Chandler 2009).
Consultants
A common theme throughout the Beaconsfield Investigation Report is the lack of clarity in the consultant process following the October 2005 rockfalls. Many of the issues relate to ground support as discussed earlier. There was disagreement between consultants about the suitability of the compressive arch design philosophy with the ground conditions at BGM. This disagreement was never formally resolved or documented. The depth of failure problem was pointed out by multiple consultants but was never acted upon or addressed by BGM.
One of the consultants brought in following the October 2005 rockfalls was, according to BGM, partly tasked with reviewing the other consultants reports and peer reviewing the ground support system. The consultant considered their brief to be to conduct a general overview of the operation and highlight some potential ideas for improvement based on his experience at different sites. This confusion about the role of the consultant appears to have led to at least one BGM manager viewing the consultant’s report as a peer review of the existing ground support system which was not actually the case. Part of the consultant’s report was an assessment of the effect of the mining sequence on seismic hazard and the loading of nearby structures. However, BGM did not brief the consultant on the structural geology at the time of his visit. The coroner found the lack of a geological briefing to be “perplexing.” The consultant was unaware of the C-HW shear when writing his report but later said that this structure would have been relevant to his advice on the mining sequence. The C-HW shear was ultimately identified as the source of the Anzac Day event.
The investigators felt that a collective meeting with all the consultants reviewing the October 2005 rockfalls should have been convened. This would have allowed for an exchange of views and an opportunity to resolve conflicting advice. There was no collective close-out meeting with the group of consultants. The other critiques were the lack of clarity about the scope of each consultants work and the decision for the auditor of the ground support system being asked to “mark their own work.”
Communication
Another common theme in the findings of the investigation was how poor communication meant that important information didn’t reach the right people. The poor communication was evident between workers and supervisors, between supervisors and management, between consultants and the technical team, and between management and the broader workforce.
Leading up to Anzac Day, multiple workers observed signs of poor ground conditions on the 925 m level. A shift supervisor noted deformed mesh in the backs and water seeping through fractured ground. He was concerned enough to instruct a bogger operator to use a larger machine for extra protection and to take an early break. Another bogger operator made a note of increased ground movement on the day-shift before the Anzac Day rockfall occurred on night-shift. A seasoned operator said that he experienced the most severe drilling conditions of his career and collapsing holes while drilling the upholes for stope 10.
None of the observations from different crew members made their way to the underground manager who acknowledged he should have been made aware of them. The investigation highlighted the lack of a formal mine foreman role, no structure to the shift handover process, and no reliable path for the responsible people to receive information key to making risk management decisions. The rock noise reporting system had largely become unused after the installation of the seismic system. Workers were under the impression that the electronic recording system had replaced the manual reporting system. Even though the manual system was designed to capture qualitative information the seismic system could not record.
Three days before Anzac Day, there was a 30-tonne fall of ground on the 980 m level accompanied by a ML+0.2 event. Two miners were working nearby at the time. According to the GCMP at BGM, this event should have been immediately reported to the underground manager, and the area should have been closed until inspected by management. Instead, the supervisor sent an email to the technical team approximately 25 hours after the event. No management inspection of the rockfall took place. The area was re-entered the next shift and rehabilitated without any authorisation from management.
While several levels below the Anzac Day rockfall, the handling of the fall of ground on the 980 m level was troubling to investigators. The coroner found this to be a direct breach of the GCMP and a clear illustration of the inadequacy of BGM’s monitoring processes in the days leading up to Anzac Day.
The report by Quinlan (2007) contains a lot of testimony from experienced members of the workforce who had genuine concerns about the seismicity and mining method at BGM prior to Anzac Day. One shift supervisor took extended leave after the October 2005 rockfalls because he believed the mine was no longer safe to work in. The underground manager confirmed receiving a handwritten note under his office door from a miner asking for a particular stope on the 815 m level to be left before someone was killed.
Much of the workforce discontent was related to the removal of the crown pillars (the upper level of each block). Many workers believed that removing crown pillars compromised the structural integrity of the mine. The level of discontent is surprising since BGM was always designed for 100 % extraction and leaving the crown pillars behind was never seriously considered. The thinking from management and geotechnical team was that leaving pillars would be a source of significant events. The resident manager stated at the inquest that he was unaware of the workforce concerns about mining methods prior to Anzac Day. Workers interviewed by the investigators frequently expressed the view that raising concerns about mining methods was pointless because they would not be treated seriously.
Another communication failure was the limited information transfer between management and the workforce on geotechnical matters. The scope and content of the consultants’ reports were not circulated around the workforce. The memo sent to workers following the October 2005 events was considerably less candid than the memo sent to the mine’s administrator. It did not state the magnitude of the event, that it was the largest ever recorded at the mine, that it represented a recent escalation in event magnitude, or that management was reviewing ground support, pillar thickness, and the mining method. It is possible that a lot of the questions the workforce had could have been readily answered by management if they had been more aware of the concerns. If the workforce was more aware of the escalation in hazard, their observational reports may have been more detailed and frequent, and more information may have made it to management and the technical team.
Risk Assessment
In some sense, the BGM response to the October 2005 rockfalls seemed strong. Production was suspended and multiple consultants were brought in to review various aspects of the operation. The resident manager sent a memo to the mine’s administrator with a clear plan of action. He set out five steps that would need to be completed before full production was resumed:
- A level-by-level audit of current ground support, assess relative to current standards
- A back-analysis and stress modelling review of the mining sequence
- Answer the geotechnical question “Are our current ground support standards sufficient for the seismicity being experienced?”, and if they aren’t, “What is required?”
- Implement any ground support upgrades that resulted from the audit and review
- Produce a new production schedule and model the new sequence
By early February 2006, mining had resumed but only two of the five steps had been completed. The stress modelling wasn’t completed until March. The questions raised in step 3 regarding ground support were never really addressed. There was no documentation to identify who made the decision to resume mining, when the decision was made, or what analysis or reasoning was used to justify the decision. The coroner found this to be a serious failure of the risk assessment process.
The failure of documentation was a central theme to all the shortcomings identified by the coroner and investigators in BGM’s risk assessment process. So many decisions; to resume mining, to reject the idea of cable bolts, the sequence reversal of stopes 8 and 10, were all made without the reason for the decision being explicitly documented. Both Quinlan (2007) and Chandler (2009) emphasise that documentation is itself a risk control measure, not just a formality. Documentation forms the basis for later reviews. Assumptions can be checked over time to ensure they are still applicable.
Key Lessons
A lot has changed about seismic risk management since the events at Beaconsfield. There are some aspects that are hard to see repeated in a modern mining environment, but there are some lessons that may still be worth emphasising, even if they are just a reminder.
-
The rockfall reports held a lot of valuable information and clear signs that there were problems with the small block size and deep failures in the backs. The investigators found no evidence of a comprehensive review of the trends in the rockfall reports. A review should have revealed the inadequate surface support and bolt embedment length. This highlights the need for regular reviews of rockfall and damage records for identifiable patterns.
-
The ground support design philosophy at BGM was built on the compressive arch theory. This approach was not suitable for the depth of failure and cohesionless failure mass that was prominent at BGM and did not consider dynamic loads. The consistent patterns in the rockfall history made it clear that the design philosophy was not appropriate at BGM.
-
The ground support at BGM was designed by a regular consultant. When a review was triggered, the same consultant was brought in as the ground support auditor. The coroner said that this was like asking someone to "mark their own work". An independent, alternate parties’ opinion is worth seeking when reviewing your existing practices.
-
A consultant was brought in to conduct a holistic assessment of the seismic hazard and mining approach at BGM, but he was not fully briefed about the local geology. There were relevant structures present that would have influenced his advice on the mining sequence. Consultants can only work with the information they are given.
-
There was a conflict between two consultant reports about the need for cable bolt support in the ore drives and the suitability of the compressive arch theory for design. BGM effectively deferred to the original ground support designer but did not document any reasoning. When there is disagreement between reports, it is important to resolve the conflict with a documented process.
-
The mining sequence was reversed for stopes 8 and 10 compared with the planned sequence that was modelled and reviewed. The sequence reversal decision was not formally assessed, not communicated to the regular consultant, and not documented. Any time the extraction sequence deviates from the approved plan, the geotechnical implications should be evaluated and documented and a new risk management plan approved.
-
There were several observations made by experienced operators and supervisors regarding the ground conditions in the days leading up to Anzac Day. The ground observation reporting system was broken and the information never made it to management. The workforce should be treated as a part of the geotechnical data collection system, through face-to-face time, structured handovers about ground conditions, and a culture that treats the reporting of observations as a valuable contribution to a safe workplace.
-
The workforce at BGM received very little information regarding the risk assessment process following the October 2005 rockfalls. They weren’t told what the seismic data showed or what the consultants found. An educated and informed workforce makes their observations more useful and meaningful. If they know what to look for, and what should be reported, their reports will likely be more detailed and frequent.
-
The Beaconsfield investigation scrutinised everything from shift plods, handwritten inspection notes, email timestamps, and the length and comprehensiveness of personal meeting notes. The reasons for making decisions like choosing one type of bolt over another, why a change in sequence was accepted, why a consultant recommendation wasn’t adopted must be documented. From the perspective of an investigator, if the reason for a decision is not documented, there is no basis to conclude that the decision was reasoned at all.
The lessons from Beaconsfield remind us that managing seismic risk involves a rigorous process, clear communication, and careful documentation of each decision. Even after all these years, those lessons remain as relevant as ever.